Are you suffering from a dull, persistent ache in your back or a sudden inability to pass urine normally? These aren’t just annoyances; they are warning signs that your body’s drainage system is failing. Ignoring the pressure building inside you could lead to permanent damage of kidney obstruction.
Dr. Prof. Aimun Ahmed, a Consultant Nephrologist with over 30 years of experience at Lancashire Teaching Hospitals, has managed more than 5,000 patients with various kidney conditions. His expertise in treating obstructive kidney disease helps patients understand their condition and receive evidence-based care tailored to their specific situation.
What Is Kidney Obstruction?
Kidney obstruction refers to any blockage that prevents urine from flowing normally through your urinary system. Your kidneys constantly filter waste from your blood, producing urine that travels down two thin tubes (ureters) into your bladder. When something blocks this pathway, urine backs up into the kidney, creating pressure that can damage delicate filtering structures.
This condition affects people differently depending on whether one or both kidneys are blocked, how severe the obstruction is, and how quickly it develops. Acute obstruction happens suddenly and requires immediate attention, while chronic blockages develop slowly over months or years.
The medical term “hydronephrosis” describes the swelling that occurs when urine accumulates in the kidney. Think of it like a water balloon filling up—the kidney stretches and expands, potentially causing permanent harm to the tissues responsible for filtering your blood.
Kidney Stones Obstruction
Ureteral stones represent the most common cause of sudden kidney blockage in adults. These hard mineral deposits form when certain substances in your urine crystallize and stick together. While many stones are tiny enough to pass without notice, larger ones can lodge in the narrow ureter, creating a complete or partial blockage.
Kidney stones lead to obstruction through several mechanisms. A stone traveling from the kidney into the ureter may get stuck at natural narrowing points—where the ureter connects to the kidney, crosses over pelvic blood vessels, or joins the bladder. The size, shape, and location of the stone determine whether it will pass on its own or require medical intervention.
Non-obstructive stones sit quietly in the kidney without blocking urine flow. These may not cause symptoms but could move at any time, suddenly transforming into an obstructing stone that triggers intense pain and potential complications. Regular monitoring helps catch these before they cause problems.
The body naturally tries to flush out stones by increasing urine production and triggering muscle contractions in the ureter. This explains why stone pain often comes in waves—the ureter squeezes rhythmically, attempting to push the blockage through. Understanding this mechanism helps patients recognize what’s happening during a stone episode.
Kidney Obstruction Causes
Beyond stones, numerous conditions can create blockages at different levels of the urinary tract. Knowing these potential causes helps identify risk factors and explains why your doctor might order specific tests.
- Congenital abnormalities present from birth include ureteropelvic junction obstruction, where the connection between the kidney and ureter forms incorrectly. This birth defect may not cause symptoms until adulthood when increased urine production or a minor injury triggers noticeable problems.
- Benign prostatic hyperplasia affects many men over 50, causing the prostate gland to enlarge and squeeze the urethra. This doesn’t directly block the ureters but increases bladder pressure, which can back up into the kidneys over time, especially if left untreated for prolonged periods.
- Tumors and masses either inside or outside the urinary tract can compress ureters. Bladder cancer, colon cancer, or gynecological tumors may press against these delicate tubes. Even benign masses like large ovarian cysts occasionally cause obstruction through external pressure.
- Strictures are scar tissue narrowings that develop after injury, infection, or medical procedures. Previous kidney stone treatment, radiation therapy, or surgical complications can create these permanent narrowings that gradually worsen.
- Blood clots rarely block the urinary tract but can occur after trauma, surgery, or in patients with bleeding disorders. These typically dissolve naturally but may require treatment if causing severe obstruction.
- Pregnancy creates temporary obstruction in some women as the growing uterus compresses the right ureter. This usually resolves after delivery but requires monitoring to prevent kidney damage during the pregnancy.
Kidney Obstruction Symptoms
Recognizing obstruction symptoms early dramatically improves outcomes. The presentation varies based on whether the blockage develops suddenly or gradually, and whether one or both kidneys are affected.
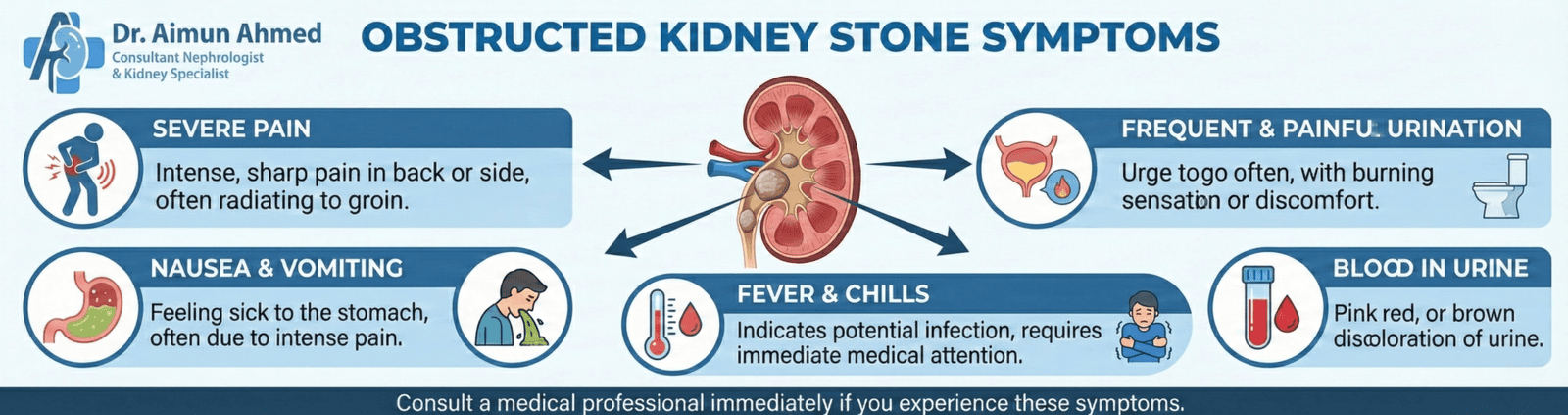
- Acute obstruction typically announces itself with severe, sudden pain. Patients describe this as the worst pain they’ve experienced—a deep, cramping sensation in the back or side that radiates toward the groin. The pain often comes in waves as the ureter contracts, attempting to push past the blockage.
- Changes in urination provide important clues. You might notice decreased urine output despite drinking normally, difficulty starting urination, or a weak stream. Some patients experience frequent urges to pee but produce very little. Blood in the urine (turning it pink, red, or brown) signals irritation or injury from a moving stone.
- Nausea and vomiting frequently accompany kidney obstruction, sometimes leading patients to think they have a stomach virus. This occurs because nerves from the kidney share pathways with those from the digestive system, creating referred symptoms.
- Fever and chills indicate infection has developed above the blockage—a medical emergency called obstructive pyelonephritis. Bacteria trapped in the backed-up urine multiply rapidly, potentially leading to sepsis, a life-threatening condition requiring immediate IV antibiotics and urgent drainage.
- Chronic obstruction produces vaguer symptoms. Patients might notice gradual fatigue, mild discomfort, or unexplained swelling. Some discover their obstruction only when blood tests reveal declining kidney function during routine checkups.
Obstructed Kidney Stone Symptoms
When kidney stones cause obstruction, symptoms intensify beyond typical stone discomfort. The blockage creates unique warning signs that distinguish it from stones that pass without incident.
- Intense, unrelenting pain characterizes obstructing stones. Unlike the intermittent discomfort of smaller stones moving through the ureter, complete obstruction often produces constant, severe pain that doesn’t improve with position changes. Patients struggle to find any comfortable position, constantly shifting and pacing.
- Contrast between sides helps identify which kidney is affected. Pain typically localizes to one side of the lower back, just below the ribs. The location may shift as the stone moves, tracking the ureter’s path from the back toward the groin area.
- Swelling and visible changes sometimes occur with severe obstruction. The affected kidney may become tender to touch, and rarely, swelling becomes visible or palpable through the abdominal wall, especially in thin individuals.
- Urinary changes specific to stones include gritty sediment, sand-like particles, or actual stone fragments in the urine. Some patients hear or feel stones “pinging” in the toilet bowl—small pieces that have broken off the main stone.
- Systemic symptoms like sweating, rapid heartbeat, and extreme restlessness accompany severe stone pain. These reflect the body’s stress response and should prompt immediate medical attention, especially if fever develops.
UPJ Kidney Obstruction
Ureteropelvic junction obstruction represents a specific anatomical problem where the renal pelvis (kidney’s collection system) connects improperly to the ureter. This congenital condition affects roughly 1 in 1,500 people, though many cases remain undiagnosed until adulthood.
The UPJ acts like a funnel, narrowing the wide renal pelvis down to the thin ureter. When this junction forms incorrectly, it creates a bottleneck that restricts urine flow. The kidney produces urine normally but can’t drain efficiently, leading to progressive swelling and pressure buildup.
- Types of UPJ obstruction include intrinsic narrowings (the junction itself is too tight) and extrinsic compression (blood vessels or bands of tissue press on the junction from outside). Some patients have intermittent obstruction that worsens with high urine production, such as after drinking lots of fluids.
- Presentation in children versus adults differs significantly. Infants and young children often show abdominal masses, failure to thrive, or urinary tract infections. Adults typically experience flank pain that worsens after drinking fluids, recurrent infections, or blood in urine. Some discover their UPJ obstruction only when imaging for another condition reveals an enlarged kidney.
- Long-term consequences without treatment include progressive loss of kidney function on the affected side. The constant pressure damages the nephrons (filtering units), and infections become more frequent as stagnant urine provides a breeding ground for bacteria. Timely treatment of kidney obstruction from UPJ prevents these complications and preserves function.
How Kidney Obstruction Affects Your Body
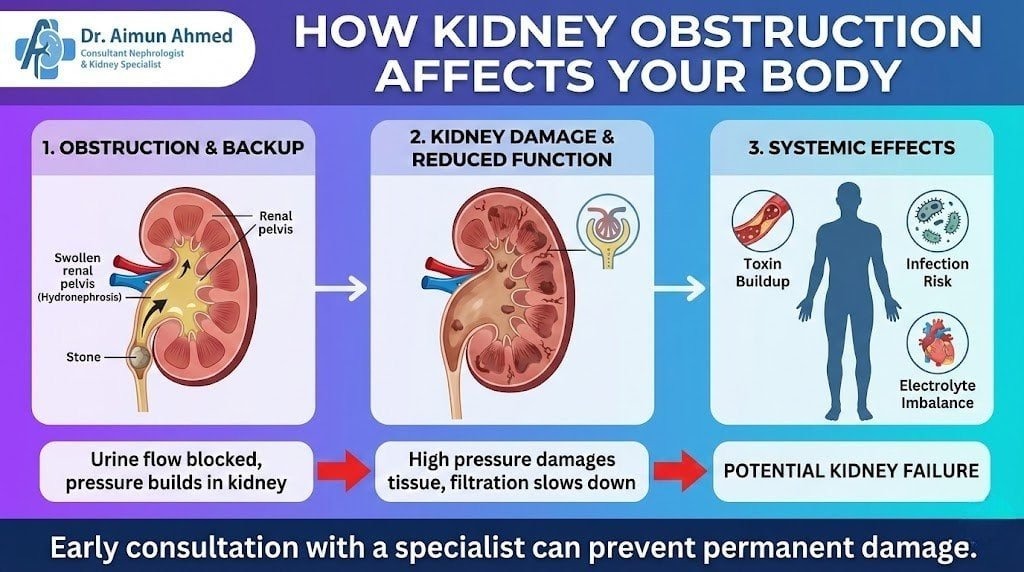
Understanding what happens inside your body during obstruction helps explain why prompt treatment matters so much. The kidneys are remarkably resilient organs, but sustained pressure causes irreversible damage surprisingly quickly.
- Pressure buildup from obstruction causes pressure buildup that works backward through the kidney’s collecting system. This increased pressure compresses blood vessels, reducing the kidney’s blood supply. With less oxygen and nutrients reaching kidney tissue, cells begin dying—a process that accelerates the longer obstruction continues.
- Acute kidney injury (AKI) develops when obstruction is severe or affects both kidneys. Waste products that should be filtered out accumulate in the bloodstream, causing nausea, confusion, and fluid retention. Potassium levels rise dangerously high, potentially affecting heart rhythm. Without intervention, AKI progresses to complete kidney failure requiring dialysis.
- Chronic kidney disease (CKD) results from prolonged partial obstruction. The kidney compensates initially, but ongoing pressure gradually destroys filtering capacity. Patients may not notice symptoms until they’ve lost over 60% of function. At this stage, reversing damage becomes impossible even after relieving the obstruction.
- Infection risks multiply when urine stagnates behind a blockage. Bacteria thrive in this environment, and the body’s immune cells can’t reach the infected area effectively. Infections can spread to the bloodstream, causing sepsis—a condition where mortality rates increase with each hour of delayed treatment.
- Compensatory changes occur when one kidney is blocked and the other is healthy. The unaffected kidney enlarges and works harder, sometimes maintaining near-normal overall function. This explains why patients with chronic one-sided obstruction may feel fine despite significant damage to the blocked kidney.
Kidney Obstruction Treatment
Treatment approaches vary dramatically based on the obstruction’s cause, severity, and duration. Dr. Ahmed emphasizes that the goal isn’t just relieving the blockage but preserving kidney function and preventing complications.
Emergency interventions for acute obstruction with infection focus on drainage first, definitive treatment later. Options include:
- Ureteral stents: thin tubes placed through a cystoscope (camera in the bladder) that thread up the ureter, providing an internal drainage channel around the blockage
- Nephrostomy tubes: catheters inserted through the skin directly into the kidney, draining urine externally into a collection bag
- Foley catheters: for bladder-level obstructions, especially from prostate enlargement
Medical management
addresses underlying causes without surgery when possible. Smaller stones under 5mm usually pass spontaneously with increased fluid intake, pain management, and medications that relax the ureter (like tamsulosin). Prostate enlargement responds to medications that shrink the gland or relax the bladder neck.
Monitoring and supportive care
includes managing pain with appropriate medications (avoiding NSAIDs if kidney function is compromised), maintaining hydration, treating infections with targeted antibiotics, and regular imaging to track stone position or assess kidney swelling.
Long-term management
for chronic conditions like UPJ obstruction or recurrent stones involves addressing root causes. This might include dietary changes to prevent stone formation, managing underlying metabolic conditions, or planned surgical correction during a stable period rather than during acute crisis.
Kidney Obstruction Surgery
When conservative treatments fail or aren’t appropriate, surgical intervention becomes necessary. Modern techniques offer excellent success rates with minimal invasiveness.
- Shock wave lithotripsy (SWL) uses focused sound waves to break stones into smaller fragments that pass more easily. Patients lie on a specialized table while the machine delivers precisely targeted shock waves through the skin. This outpatient procedure works best for stones under 2cm in favorable locations, though success varies with stone composition.
- Ureteroscopy involves threading a thin scope through the urethra and bladder up into the ureter. The surgeon visualizes the stone directly and uses laser energy to fragment it or removes it with tiny baskets. This procedure allows treatment of stones anywhere in the ureter or kidney, with excellent success rates and same-day discharge for most patients.
- Percutaneous nephrolithotomy (PCNL) tackles larger kidney stones through a small incision in the back. The surgeon creates a tunnel directly into the kidney, allowing removal of substantial stone burdens that other procedures can’t address. This requires a brief hospital stay but provides definitive treatment for complex cases.
- Pyeloplasty corrects UPJ obstruction by removing the narrowed junction and reconnecting the ureter to the renal pelvis. Minimally invasive (laparoscopic or robotic) approaches have largely replaced open surgery, reducing recovery time from weeks to days while maintaining success rates above 95%.
- Prostate surgery relieves bladder outlet obstruction through various techniques. Transurethral resection (TURP) removes prostate tissue blocking the urethra, while newer procedures like laser enucleation offer similar results with less bleeding and faster recovery.
- Risks and complications of surgical intervention include bleeding, infection, urine leaking from the kidney or ureter, injury to surrounding structures, and need for additional procedures. However, complication rates remain low in experienced hands, and the benefits of relieving significant obstruction far outweigh these risks.
Diagnosis and Detection
Accurate diagnosis requires combining clinical assessment with appropriate imaging and laboratory tests. The diagnostic approach depends on symptom severity and whether you’re experiencing your first episode or have a history of kidney problems.
Initial evaluation starts with a detailed history and physical examination. Your doctor will ask about pain characteristics, urinary changes, previous stones, family history, and risk factors. Physical examination includes checking for tenderness over the kidneys and assessing for fever or signs of dehydration.
Laboratory testing provides crucial information:
- Urinalysis detects blood, infection, or crystals
- Blood tests measure kidney function (creatinine, BUN), electrolytes, and infection markers
- Urine culture identifies specific bacteria if infection is suspected
Ultrasound offers a quick, radiation-free way to visualize kidney swelling (hydronephrosis). It works well for detecting obstruction but may miss small stones and doesn’t always show the exact blockage location. Ultrasound is particularly valuable in pregnancy and children.
CT scanning without contrast provides the gold standard for kidney stone detection and obstruction evaluation. This quick, highly accurate test shows stone size, location, and density while revealing alternative diagnoses. Modern protocols minimize radiation exposure while maintaining excellent image quality.
Additional imaging may include:
- Intravenous pyelogram (IVP): contrast dye study showing urinary tract anatomy
- MRI: useful when radiation exposure should be avoided
- Nuclear scans: assess individual kidney function and drainage
Functional testing like a diuretic renogram helps determine whether borderline findings represent true obstruction or just anatomical variation. This becomes particularly important when considering surgery for conditions like UPJ obstruction.
Prevention and Risk Management
While not all causes of kidney obstruction are preventable, many strategies reduce your risk or catch problems early when they’re most treatable.
Stone prevention depends on stone type but generally includes:
- Drinking enough water to produce 2-3 liters of urine daily
- Limiting sodium intake (increases calcium in urine)
- Adequate but not excessive calcium intake (dietary calcium actually reduces stone risk)
- Reducing animal protein consumption if prone to uric acid stones
- Addressing metabolic conditions that promote stone formation
Medical management of underlying conditions prevents secondary obstruction. This includes treating prostate enlargement before it causes kidney damage, controlling urinary tract infections that could lead to strictures, and monitoring conditions that increase stone risk.
Regular monitoring for high-risk patients includes periodic imaging and kidney function testing. Those with a history of stones, known anatomical abnormalities, or single kidney require closer surveillance to catch problems early.
Recognizing warning signs allows prompt treatment before significant damage occurs. Seek immediate medical attention for severe flank pain, fever with urinary symptoms, inability to urinate, or blood in urine with significant discomfort.
Living with Kidney Obstruction
For patients with chronic or recurrent obstruction, understanding how to manage the condition improves quality of life and reduces complications.
- Lifestyle modifications help prevent recurrence. Beyond dietary changes for stone prevention, patients learn to recognize their individual triggers. Some notice flare-ups after dehydration, certain foods, or even specific activities.
- Managing stents or tubes requires proper care to prevent infection and ensure continued function. Patients with long-term stents need regular replacement every 3-6 months. Nephrostomy tubes require daily flushing and careful site care. Understanding warning signs of malfunction (pain, fever, decreased drainage) prevents emergencies.
- Planning ahead includes carrying medical information about your condition, knowing which hospitals have urology coverage, and having a plan for managing acute episodes. Patients with recurrent stones often keep pain medication available and know when they need emergency versus urgent evaluation.
- Psychological impact shouldn’t be underestimated. Chronic pain, recurrent procedures, and uncertainty about future episodes create stress and anxiety. Connecting with support groups, working with mental health professionals when needed, and maintaining open communication with your medical team all contribute to better coping.
When to Seek Emergency Care
Certain situations require immediate medical attention rather than scheduling an appointment with your regular doctor. Understanding these helps you make appropriate decisions quickly.
Seek emergency care immediately if you experience:
- Fever (over 100.4°F/38°C) combined with flank pain or urinary symptoms
- Inability to urinate for more than 6 hours with bladder fullness
- Severe pain not controlled with over-the-counter medications
- Persistent vomiting preventing fluid intake
- Confusion, extreme weakness, or rapid heartbeat with known kidney problems
- Only one functioning kidney with symptoms of obstruction
Urgent (same-day) evaluation needed for:
- New onset of blood in urine with pain
- Severe pain that comes and goes
- Symptoms suggesting stone passage
- Worsening pain despite previous treatment
Routine follow-up appropriate for:
- Mild intermittent discomfort without fever
- Known small stones being monitored
- Scheduled stent changes or post-procedure checks
Understanding these distinctions prevents both delayed care when emergencies occur and unnecessary emergency visits for conditions that can wait for regular appointments.
Frequently Asked Questions
What causes kidney obstruction?
Kidney obstruction results from anything blocking urine flow from the kidneys to the bladder. The most common cause in adults is ureteral stones that lodge in the narrow ureter. Other causes include congenital abnormalities like ureteropelvic junction obstruction, enlarged prostate in men, tumors compressing the urinary tract, scar tissue from previous injuries or infections, blood clots, and pregnancy-related compression.
Each person’s situation is unique, so proper diagnosis identifies the specific cause and guides treatment.
How to remove blockage in kidneys?
Removing kidney blockages depends on the underlying cause. Smaller stones often pass naturally with increased fluids and pain management. Larger stones may require procedures like shock wave lithotripsy to fragment them, ureteroscopy to remove them directly, or percutaneous surgery for very large stones.
Structural problems like UPJ obstruction need surgical reconstruction. Prostate-related blockages respond to medications or surgical procedures that reduce prostate size. Emergency situations may require temporary drainage with stents or nephrostomy tubes before definitive treatment.
What happens when your kidneys are blocked?
When kidneys are blocked, urine backs up into the kidney, creating pressure that damages delicate filtering structures. Initially, you might experience severe pain, decreased urination, and swelling in the affected kidney.
If both kidneys are blocked or you have only one functioning kidney, waste products accumulate in your blood, causing nausea, confusion, and dangerous electrolyte imbalances. Without prompt treatment, temporary acute kidney injury can progress to permanent chronic kidney disease. Infection above a blockage creates life-threatening sepsis requiring emergency intervention.
What are the first signs of kidney stones?
The first signs of kidney stones vary depending on stone size and location. Many people notice sudden, severe pain in their side or back below the ribs that may radiate toward the groin. The pain typically comes in waves as the ureter contracts.
You might see blood in your urine (pink, red, or brown color), experience frequent urges to urinate with small amounts produced, or notice burning during urination. Nausea, vomiting, and inability to find a comfortable position are common. Some stones cause no symptoms until they start moving.
What is an obstruction of the kidney stones?
An obstruction of the kidney stones occurs when a stone blocks the ureter, preventing urine from flowing from the kidney to the bladder. This differs from non-obstructive stones that sit in the kidney without blocking drainage. Obstructing stones create pressure buildup in the kidney, causing severe pain and potential damage.
The blockage location—whether at the ureteropelvic junction, mid-ureter, or where the ureter enters the bladder—affects symptoms and treatment options. Complete obstruction requires more urgent intervention than partial blockages.
Do obstructing kidney stones need to be removed?
Not all obstructing kidney stones need removal—the decision depends on several factors. Stones under 5mm often pass spontaneously within days to weeks with supportive care. However, immediate removal becomes necessary if infection develops above the obstruction, pain remains uncontrolled despite medication, the kidney shows signs of significant damage, or the stone fails to progress after a reasonable observation period.
Larger stones (over 7mm) rarely pass on their own and typically require intervention. Your doctor weighs stone size, location, symptoms, and kidney function when recommending treatment.
How to tell if a kidney stone is obstructed?
Signs of an obstructed kidney stone include severe, constant pain that doesn’t improve with position changes, decreased urine output despite normal fluid intake, visible swelling or tenderness over the affected kidney, and worsening symptoms over hours.
Imaging provides definitive diagnosis—ultrasound shows kidney swelling (hydronephrosis), while CT scan reveals the stone’s exact location and whether it’s causing complete or partial blockage.
The presence of fever with these symptoms suggests infection and requires emergency treatment. Any suspicion of obstruction warrants prompt medical evaluation.
How long can a kidney stone stay obstructed?
The safe duration of kidney stone obstruction varies based on completeness of blockage and presence of infection. Complete obstruction begins damaging kidney tissue within hours, with irreversible damage possible after 1-2 weeks.
Partial obstruction allows some drainage and may persist longer without permanent damage, but still requires treatment within days to weeks. Infection above an obstruction creates an emergency—even hours of delay increases complication risks. Generally, doctors aim to relieve significant obstruction within 24-48 hours of diagnosis, either through stone removal or temporary drainage procedures.
How serious is kidney obstruction?
Kidney obstruction severity ranges from manageable to life-threatening depending on several factors. Complete obstruction of both kidneys or your only functioning kidney requires emergency treatment to prevent kidney failure. One-sided obstruction with a healthy opposite kidney is less critical but still needs prompt attention to preserve the affected kidney.
The presence of infection elevates any obstruction to an emergency. Chronic partial obstruction causes gradual, often irreversible damage. Timely treatment of kidney obstruction prevents these serious complications and preserves long-term kidney health.
How do they remove an obstructed kidney stone?
Doctors remove obstructed kidney stones through several approaches based on stone characteristics. Ureteroscopy, the most common procedure, uses a thin scope passed through the bladder up to the stone, which is then fragmented with a laser or removed with small baskets.
Shock wave lithotripsy breaks stones into passable fragments using focused sound waves from outside the body. Larger stones may require percutaneous nephrolithotomy—surgery through a small back incision directly into the kidney. Emergency situations often involve placing a temporary stent or nephrostomy tube for drainage before definitive stone removal.
Is an obstructing kidney stone an emergency?
An obstructing kidney stone becomes an emergency when accompanied by fever, affecting both kidneys or a single functioning kidney, or causing uncontrolled pain. These situations require immediate hospital evaluation and treatment, often including IV fluids, antibiotics if infection is present, and urgent drainage or stone removal.
Uncomplicated obstruction without these features is urgent but not always an emergency—it requires evaluation within 24 hours. The key is recognizing warning signs: fever with flank pain signals potential sepsis requiring emergency care regardless of other factors.
How big is an obstructing kidney stone?
Obstructing kidney stones vary in size, but stones larger than 5mm have higher obstruction risk. The critical size depends on location—stones at the ureteropelvic junction may obstruct at 6-7mm, while those at the ureterovesical junction (where ureter meets bladder) may block at smaller sizes due to narrower anatomy.
Even 3-4mm stones occasionally obstruct if they impact at a narrow point. Stone shape also matters—irregular, jagged stones are more likely to get stuck than smooth, round ones. Treatment urgency depends more on obstruction degree than absolute stone size.
What’s the worst type of kidney stone to have?
Cystine stones are often considered the most challenging kidney stone type. These form in people with a genetic disorder causing excessive cystine in urine. They grow large, recur frequently, and resist standard treatments like shock wave lithotripsy.
Struvite stones (infection stones) also pose serious problems because they grow rapidly, form complex shapes that fill the kidney’s collecting system, and require complete removal to prevent recurrent infections.
Calcium oxalate monohydrate stones are extremely hard and resist fragmentation. The “worst” stone depends on individual circumstances—any type causing recurrent obstruction and loss of kidney function is serious.
What happens when the stones cause an obstruction?
When stones cause an obstruction, urine flow stops or slows significantly, creating pressure that backs up into the kidney. This pressure triggers severe pain as the kidney swells and the ureter spasms trying to push the stone through. The backed-up urine provides an environment for bacterial growth, increasing infection risk.
Pressure compresses blood vessels feeding the kidney, reducing oxygen and nutrient delivery to kidney tissue. Without relief, cells begin dying, leading to permanent function loss. The body may produce less urine overall, and waste products accumulate in the blood. Emergency intervention focuses on relieving pressure and preventing irreversible damage.
Taking Control of Kidney Health
Kidney obstruction represents a spectrum of conditions from simple, self-resolving stones to complex anatomical problems requiring surgical correction. The common thread is the importance of early recognition and appropriate treatment. Whether you’re experiencing your first episode of kidney pain or managing chronic obstruction, understanding your condition empowers you to make informed decisions about your care.
Dr. Prof. Aimun Ahmed’s three decades of experience have shown that most patients achieve excellent outcomes when obstruction is diagnosed and treated promptly. Modern diagnostic tools identify problems quickly, and minimally invasive treatments preserve kidney function while minimizing discomfort and recovery time. The key is recognizing warning signs and seeking appropriate care without delay.
For patients with recurrent issues, working with experienced specialists like Dr. Ahmed ensures comprehensive management that addresses not just the immediate obstruction but underlying causes and prevention strategies. This holistic approach—combining cutting-edge medical treatment with practical lifestyle modifications—offers the best path to maintaining healthy kidneys for life.
Remember that your kidneys are remarkably resilient organs, but sustained obstruction can cause irreversible damage surprisingly quickly. Trust your symptoms, seek prompt evaluation when concerning signs appear, and work with your healthcare team to develop a treatment plan that preserves your kidney function and quality of life.