
Your kidneys work tirelessly every day, filtering roughly 200 quarts of blood to remove waste and excess fluid. But what happens when your body’s own defense system mistakes these vital organs for foreign invaders? This is the reality for thousands of people living with autoimmune kidney disease—a condition where the immune system, designed to protect you, instead launches an attack against your kidneys.
Reality television fans were recently moved when Bethenny Frankel shared her stage 2 chronic kidney disease diagnosis, with doctors investigating potential autoimmune causes. Her openness sparked important conversations about autoimmune kidney disease.
The complexity of autoimmune kidney disease lies in its deceptive nature. Unlike a broken bone or visible wound, kidney damage often progresses silently, with symptoms appearing only after significant harm has occurred. Understanding these conditions isn’t just about medical knowledge—it’s about recognizing warning signs early, seeking proper diagnosis, and working with specialists who can help preserve kidney function before irreversible damage takes hold.
Whether you’ve just received a diagnosis, noticed concerning symptoms, or simply want to understand more about autoimmune kidney disease, this comprehensive guide will walk you through everything you need to know. From the most common types to cutting-edge treatments, we’ll explore how autoimmune conditions affect the kidneys and what you can do to protect your health.
Understanding Autoimmune Disease and Kidney Function
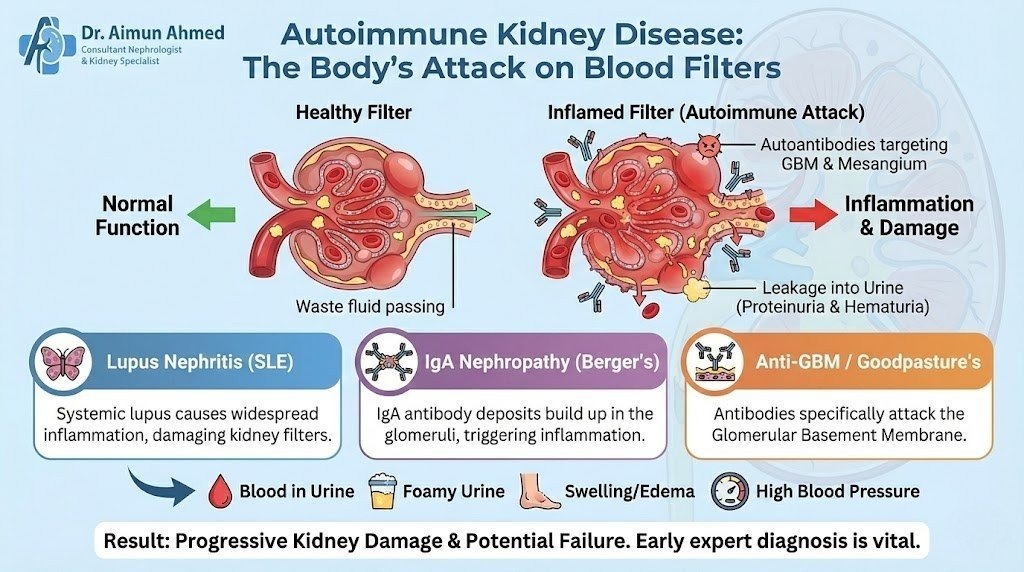
Before diving into specific conditions, let’s establish what happens when autoimmunity targets the kidneys. Your immune system normally produces antibodies to fight off bacteria, viruses, and other harmful invaders. In autoimmune disease, however, the body mistakenly creates autoantibodies that attack healthy tissues instead.
The kidneys filter blood through millions of tiny structures called nephrons. Each nephron contains a glomerulus—a cluster of blood vessels that acts like a sieve, allowing waste to pass through while keeping essential proteins and cells in your bloodstream. When autoantibodies attack kidney tissue, they trigger inflammation and damage these delicate filtering structures.
This inflammatory process can lead to several problems:
- Protein leaking into urine (proteinuria)
- Blood appearing in urine (hematuria)
- Reduced filtering capacity
- Buildup of waste products in the blood
- High blood pressure
- Fluid retention and swelling
The kidneys have remarkable resilience, but chronic inflammation gradually destroys their ability to function. This is why early detection matters so much. Prof. Aimun Ahmed, a Consultant Nephrologist with over three decades of experience at Lancashire Teaching Hospitals, emphasizes that catching autoimmune kidney disease in its early stages can make the difference between preserving kidney function and progressing to renal failure.
List of Autoimmune Kidney Diseases
Several autoimmune conditions can directly or indirectly damage the kidneys. Understanding the range of these diseases helps patients and healthcare providers identify potential risks.
Lupus Nephritis
Lupus nephritis represents one of the most common forms of autoimmune kidney disease. This condition develops in people with systemic lupus erythematosus (SLE), a disease where the immune system attacks multiple organs. Approximately 40% of adults with lupus and 60% of children with lupus will develop nephritis.
The inflammation caused by lupus nephritis can affect different parts of the kidney, leading to various severity levels. Some patients experience mild kidney involvement, while others face rapidly progressive disease requiring aggressive treatment.
IgA Nephropathy
IgA nephropathy occurs when immunoglobulin A (IgA) antibodies build up in the kidneys. These antibodies normally help fight infections, but their accumulation in kidney tissue triggers inflammation. This condition often develops slowly over years, though some people experience rapid progression.
Episodes of visible blood in urine often follow respiratory infections, earning IgA nephropathy the nickname “synpharyngitic hematuria.” The disease can affect people of all ages but most commonly appears in males during their teens to thirties.
Goodpasture Syndrome
This rare but severe condition involves antibodies attacking both the kidneys and lungs. The immune system mistakenly targets a specific protein found in kidney glomeruli and lung air sacs. Without prompt treatment, Goodpasture syndrome can quickly lead to kidney failure and life-threatening lung bleeding.
Membranous Nephropathy
In membranous nephropathy, antibodies attack proteins on kidney cells, causing the filtering membranes to thicken. This leads to protein loss in urine and can progress to chronic kidney disease. While some cases occur without a clear trigger, others develop alongside autoimmune conditions like lupus.
Anti-GBM Disease
Anti-glomerular basement membrane (anti-GBM) disease happens when antibodies attack the basement membrane of kidney glomeruli. This condition can exist alone or as part of Goodpasture syndrome when lung involvement occurs.
Autoimmune Conditions with Kidney Involvement
Several systemic autoimmune diseases can affect kidney function:
- Scleroderma (affecting connective tissue and organs)
- Sjögren’s syndrome (damaging moisture-producing glands and potentially kidneys)
- Rheumatoid arthritis (occasionally involving kidney inflammation)
- Vasculitis (inflammation of blood vessels, including those in kidneys)
Symptoms of Autoimmune Kidney Disease
Recognizing symptoms early gives you the best chance of preventing serious kidney damage. Unfortunately, kidney disease often develops silently, earning its reputation as a “silent killer.” Many people don’t experience obvious symptoms until significant damage has occurred.
Early Warning Signs
Watch for these initial indicators:
Changes in Urination
- Foamy or bubbly urine (indicating protein loss)
- Pink, red, or cola-colored urine (suggesting blood)
- Increased nighttime urination
- Difficulty urinating or decreased output
Physical Symptoms
- Swelling in legs, ankles, feet, or face
- Persistent fatigue not relieved by rest
- Unexplained weight changes
- Metallic taste in mouth
- Decreased appetite
Advanced Symptoms
As kidney function declines, additional symptoms may develop:
- Nausea and vomiting
- Muscle cramps
- Persistent itching
- Shortness of breath
- Confusion or difficulty concentrating
- Sleep disturbances
- High blood pressure
Systemic Autoimmune Symptoms
Since many autoimmune kidney diseases occur alongside broader immune conditions, you might experience:
- Joint pain and swelling
- Skin rashes (particularly the butterfly rash seen in lupus)
- Persistent low-grade fever
- Hair loss
- Sensitivity to sunlight
- Mouth sores
- Chest pain when breathing deeply
Mount Sinai specialists note that symptom patterns vary significantly between different autoimmune kidney diseases. Some patients experience sudden, severe symptoms, while others notice gradual changes over months or years.
Autoimmune Kidney Disease Diagnosis
Accurate diagnosis requires a combination of clinical evaluation, laboratory tests, and sometimes kidney biopsy. The diagnostic process helps determine which specific condition you’re facing and guides treatment decisions.
Initial Assessment
Your healthcare provider will start with a detailed medical history and physical examination. They’ll ask about:
- Current symptoms and their duration
- Family history of autoimmune or kidney disease
- Recent infections or illnesses
- Medications and supplements
- Previous health conditions
Laboratory Tests
Blood and urine tests provide crucial information about kidney function and immune activity:
Blood Tests
- Creatinine and blood urea nitrogen (BUN) to assess filtering function
- Estimated glomerular filtration rate (eGFR) to stage kidney disease
- Complete blood count to check for anemia
- Albumin levels to detect protein loss
- Autoantibody panels (ANA, anti-dsDNA, ANCA, anti-GBM)
- Complement levels (C3, C4)
Urine Tests
- Urinalysis to detect blood, protein, or abnormal cells
- Protein-to-creatinine ratio
- 24-hour urine collection for protein quantification
- Urine microscopy to examine sediment
Imaging Studies
Ultrasound, CT scans, or MRI may help evaluate:
- Kidney size and structure
- Blood flow patterns
- Presence of obstruction or masses
- Complications like kidney stones
Kidney Biopsy
When other tests suggest autoimmune kidney disease but don’t provide a definitive diagnosis, kidney biopsy becomes necessary. During this procedure, a specialist removes a small tissue sample for microscopic examination.
Biopsy reveals:
- Specific type and severity of kidney damage
- Presence and pattern of immune deposits
- Degree of scarring or chronic changes
- Optimal treatment approach
Prof. Aimun Ahmed notes that biopsy results often change treatment plans, making this diagnostic tool invaluable for managing complex cases. The procedure carries minimal risks when performed by experienced specialists.
How Do You Diagnose Lupus Nephritis?
Lupus nephritis diagnosis follows a specific pathway since it occurs as a complication of systemic lupus erythematosus. Many patients already carry a lupus diagnosis when kidney involvement develops, though nephritis occasionally appears as the first lupus symptom.
Screening for Kidney Involvement
People with lupus should undergo regular kidney monitoring through:
- Urinalysis at each doctor visit
- Blood pressure checks
- Periodic blood tests for creatinine and complement levels
- Assessment of lupus disease activity
Diagnostic Criteria
Doctors suspect lupus nephritis when patients with lupus develop:
- Persistent proteinuria (protein in urine)
- Active urine sediment (blood cells, casts)
- Rising creatinine levels
- Declining complement levels
- High anti-dsDNA antibody levels
Kidney Biopsy Classification
Kidney biopsy remains the gold standard for diagnosing and classifying lupus nephritis. Pathologists categorize the disease into six classes based on the pattern and severity of kidney damage:
- Class I: Minimal changes
- Class II: Mild involvement
- Class III: Focal inflammation
- Class IV: Diffuse inflammation (most severe)
- Class V: Membranous pattern
- Class VI: Advanced scarring
This classification system guides treatment intensity and helps predict outcomes. Class III and IV lupus nephritis require the most aggressive therapy, while Class V may respond to different medications.
What Is the Most Common Autoimmune Kidney Disease?
IgA nephropathy holds the title of most common primary autoimmune kidney disease worldwide, though prevalence varies by region. In Asian countries, particularly Japan and Singapore, IgA nephropathy accounts for up to 40% of all primary kidney diseases. In Western countries, rates are lower but still significant.
However, when considering secondary autoimmune kidney diseases—those occurring as complications of other conditions—lupus nephritis becomes extremely common. Among people with systemic lupus erythematosus, kidney involvement is one of the most frequent and serious complications.
The prevalence of different autoimmune kidney diseases depends on several factors:
Geographic Variation Certain populations show higher rates of specific conditions. IgA nephropathy is more common in people of Asian descent, while lupus nephritis affects African American, Hispanic, and Asian individuals more frequently than white populations.
Age and Gender Many autoimmune diseases show gender preferences. Lupus, including lupus nephritis, affects women nine times more often than men. Goodpasture syndrome tends to affect younger males more frequently.
Genetic Factors Family history increases risk for most autoimmune conditions. Having a relative with lupus, IgA nephropathy, or other autoimmune diseases raises your chances of developing similar conditions.
Understanding prevalence patterns helps healthcare providers maintain appropriate vigilance. Prof. Aimun Ahmed recommends that people with autoimmune disease risk factors undergo regular kidney screening, even without symptoms.
Autoimmune Kidney Disease Treatment
Treatment approaches vary based on the specific condition, severity, and rate of progression. The primary goals include reducing inflammation, preserving kidney function, managing symptoms, and preventing complications.
Immunosuppressive Medications
These drugs reduce immune system activity to stop the attack on kidney tissue:
Corticosteroids Prednisone and methylprednisolone quickly reduce inflammation. Doctors often start with high doses during active disease, then taper to lower maintenance levels. Long-term steroid use requires monitoring for side effects like bone loss, diabetes, and infections.
Cytotoxic Agents Medications like cyclophosphamide and mycophenolate mofetil suppress immune cell production. These powerful drugs treat severe cases, particularly Class III and IV lupus nephritis.
Calcineurin Inhibitors Tacrolimus and cyclosporine block specific immune pathways. These medications help in certain types of kidney disease, particularly membranous nephropathy.
Newer Biologic Therapies Rituximab targets specific immune cells and shows promise in treating various autoimmune kidney diseases. Belimumab, approved for lupus, may help prevent lupus nephritis progression.
Supportive Treatments
Beyond immunosuppression, several therapies protect remaining kidney function:
Blood Pressure Control ACE inhibitors and ARBs not only lower blood pressure but also reduce protein loss and slow kidney disease progression. Target blood pressure is typically below 130/80 mmHg.
Managing Complications
- Diuretics to reduce fluid retention
- Phosphate binders to control mineral levels
- Erythropoietin-stimulating agents for anemia
- Vitamin D supplementation for bone health
Lifestyle Modifications
Daily choices significantly impact disease progression:
Dietary Adjustments Working with dietitians helps optimize nutrition while protecting kidneys. Recommendations may include:
- Limiting sodium to reduce blood pressure and swelling
- Monitoring protein intake based on kidney function stage
- Restricting phosphorus and potassium in advanced disease
- Staying well-hydrated unless fluid restrictions apply
Activity and Exercise Regular physical activity helps control blood pressure, maintain healthy weight, and improve overall wellbeing. Patients should discuss appropriate exercise levels with their healthcare team.
Avoiding Kidney Stressors
- Limiting NSAIDs (ibuprofen, naproxen)
- Avoiding unnecessary antibiotics
- Managing blood sugar if diabetic
- Quitting smoking
- Moderating alcohol consumption
Advanced Interventions
When kidney disease progresses despite treatment, additional options become necessary:
Plasmapheresis This procedure filters antibodies from blood plasma. It’s used in severe cases like Goodpasture syndrome or rapidly progressive kidney disease.
Dialysis If kidneys fail despite treatment, dialysis removes waste products and excess fluid. Options include hemodialysis (using a machine) or peritoneal dialysis (using the abdominal lining).Kidney Transplant For end-stage kidney disease, transplantation offers the best quality of life. However, autoimmune conditions may recur in the transplanted kidney, requiring continued immunosuppression.
Is Autoimmune Kidney Disease Curable?
The question of cure depends heavily on the specific condition and individual circumstances. Most autoimmune kidney diseases are chronic conditions requiring long-term management rather than offering permanent cure.
Factors Affecting Outcomes
Disease Type Some conditions respond better to treatment than others. IgA nephropathy may go into remission in some patients, while others experience slow progression. Goodpasture syndrome can sometimes be stopped with aggressive early treatment, though kidney damage may be permanent.
Timing of Treatment Early intervention dramatically improves outcomes. Starting treatment before significant scarring occurs gives the best chance of preserving kidney function. Once scarring develops, reversal becomes impossible, though progression may be slowed.
Treatment Response Individual responses to therapy vary widely. Some patients achieve complete remission with minimal medication, while others require multiple drugs and still experience disease activity.
Remission vs. Cure
Healthcare providers distinguish between remission and cure:
Complete Remission The disease becomes inactive with normal kidney function, minimal or no proteinuria, and inactive urine sediment. Patients in complete remission may reduce or stop medications, though careful monitoring continues.
Partial Remission Kidney function stabilizes and inflammation decreases, but some abnormalities persist. These patients typically continue maintenance therapy.
Active Disease Despite treatment, inflammation and kidney damage continue. These cases require treatment adjustments or alternative therapies.
Long-term Outlook
With modern treatments, many people with autoimmune kidney disease maintain good kidney function for decades. Regular monitoring, medication compliance, and lifestyle management all contribute to better outcomes.
Prof. Aimun Ahmed has managed over 5,000 patients through various stages of kidney disease, noting that those who actively participate in their care—attending appointments, taking medications as prescribed, and making lifestyle changes—consistently achieve better results than those who don’t.
Autoimmune Kidney Disease Life Expectancy
Life expectancy with autoimmune kidney disease varies tremendously based on multiple factors. Modern treatments have dramatically improved outcomes compared to even two decades ago.
Prognostic Factors
Several elements influence long-term survival:
- Kidney Function at Diagnosis People diagnosed early, before significant damage occurs, have much better prognoses. Those presenting with advanced kidney disease face more challenges.
- Disease Severity and Type Mild IgA nephropathy may not affect lifespan at all, while aggressive lupus nephritis or rapidly progressive glomerulonephritis requires intensive treatment to prevent organ failure.
- Treatment Response Patients achieving remission with treatment enjoy near-normal life expectancy. Those with resistant disease face higher risks of kidney failure and cardiovascular complications.
- Cardiovascular Health Heart disease and stroke represent major threats to people with kidney disease. Controlling blood pressure, cholesterol, and diabetes significantly improves survival.
- Compliance with Treatment Following medical recommendations, attending appointments, and taking medications as prescribed dramatically affects outcomes.
Stage-Specific Considerations
- Stages 1-3 Chronic Kidney Disease With proper management, many patients maintain stable kidney function for years or decades. Life expectancy may be minimally affected.
- Stage 4 Chronic Kidney Disease Advanced disease increases health risks, but many people live for years with careful medical management and preparation for kidney replacement therapy.
- Stage 5 (Kidney Failure) Dialysis or transplantation becomes necessary. Five-year survival rates on dialysis range from 35-50%, while kidney transplant recipients have much better outcomes, with 5-year survival exceeding 90%.
Quality of Life Considerations
Beyond lifespan, quality of life matters greatly. Many people with autoimmune kidney disease live full, active lives with appropriate treatment. Fatigue and medication side effects can challenge daily activities, but working closely with specialists helps optimize both function and wellbeing.
Autoimmune Kidney Disease in Children
When autoimmune kidney disease affects children, it presents unique challenges for patients, families, and healthcare providers. Pediatric autoimmune kidney disease differs from adult disease in several important ways.
Common Pediatric Autoimmune Kidney Diseases
Lupus Nephritis Children with systemic lupus erythematosus develop kidney involvement more frequently than adults—up to 60% of pediatric lupus patients develop nephritis. Childhood-onset lupus nephritis tends to be more severe and requires aggressive treatment.
- IgA Nephropathy Though less common in young children, IgA nephropathy can affect school-age children and teenagers. Boys are affected more often than girls.
- Henoch-Schönlein Purpura Nephritis This condition typically affects children aged 3-10 years. It causes a characteristic skin rash, joint pain, abdominal pain, and kidney inflammation. Most children recover fully, though some develop chronic kidney disease.
- Hemolytic Uremic Syndrome While often triggered by infection rather than pure autoimmunity, this condition involves immune processes attacking kidney blood vessels. It represents a leading cause of acute kidney failure in children.
Diagnosis Challenges
Recognizing kidney disease in children requires vigilance since symptoms may be subtle:
- Children may not communicate symptoms clearly
- Behavioral changes can indicate feeling unwell
- Swelling might be attributed to other causes
- High blood pressure often lacks symptoms
- Growth delays might be the first sign
Routine well-child visits should include urinalysis to catch kidney abnormalities early.
Treatment Considerations
Treating children requires balancing disease control with minimizing treatment effects on growth and development:
- Growth and Development Chronic steroid use can affect height, bone development, and puberty. Specialists work to use the lowest effective doses and incorporate steroid-sparing medications when possible.
- Educational Impact Frequent medical appointments, fatigue, and medication side effects can affect school attendance and performance. Schools may need to provide accommodations.
- Psychosocial Support Children and adolescents may struggle emotionally with chronic illness. Addressing mental health needs is crucial for overall wellbeing.
- Family Dynamics Autoimmune kidney disease affects entire families. Parents need support managing complex medical regimens while allowing age-appropriate independence.
Long-term Outlook
With advances in pediatric nephrology, most children with autoimmune kidney disease can expect to reach adulthood with functioning kidneys. However, transition to adult care represents a vulnerable period requiring careful planning.
Prof. Aimun Ahmed emphasizes the importance of establishing care with adult specialists experienced in managing patients with childhood-onset disease, as their needs often differ from those with adult-onset conditions.
Autoimmune Kidney Disease Blood Tests
Blood tests serve as essential tools for diagnosing autoimmune kidney disease, monitoring disease activity, and guiding treatment decisions. Understanding what these tests measure helps patients actively participate in their care.
Kidney Function Tests
- Serum Creatinine This waste product from muscle metabolism should be filtered by healthy kidneys. Rising creatinine levels indicate declining kidney function. Normal ranges vary by age, gender, and muscle mass.
- Blood Urea Nitrogen (BUN) Another waste product that accumulates when kidneys aren’t filtering properly. The BUN-to-creatinine ratio helps distinguish kidney disease from dehydration or other conditions.
- Estimated Glomerular Filtration Rate (eGFR) Calculated from creatinine, age, gender, and race, eGFR estimates what percentage of normal kidney function remains. It’s the primary measure for staging chronic kidney disease:
- Stage 1: eGFR >90 (normal or high)
- Stage 2: eGFR 60-89 (mild decrease)
- Stage 3: eGFR 30-59 (moderate decrease)
- (Stage 4: eGFR 15-29 (severe decrease
- Stage 5: eGFR <15 (kidney failure)
Autoimmune Markers
- Antinuclear Antibodies (ANA) A screening test for autoimmune disease. Positive ANA occurs in lupus, Sjögren’s syndrome, and other conditions. However, some healthy people test positive, so additional tests are needed.
- Anti-Double-Stranded DNA (anti-dsDNA) More specific for lupus than ANA. High levels correlate with lupus activity, particularly kidney involvement.
- Complement Levels (C3, C4) These proteins are part of the immune system. Low levels in lupus patients often indicate active disease, especially lupus nephritis.
- Antineutrophil Cytoplasmic Antibodies (ANCA) These antibodies appear in vasculitis affecting the kidneys. Two types exist: c-ANCA and p-ANCA, each associated with different vasculitis forms.
- Anti-GBM Antibodies Specific for anti-GBM disease and Goodpasture syndrome. Their presence indicates these serious conditions requiring urgent treatment.
- Cryoglobulins Abnormal proteins that can deposit in kidney blood vessels, causing inflammation and damage.
Additional Blood Tests
Complete Blood Count (CBC) Checks for anemia (common in kidney disease), infection, or other blood abnormalities.
Comprehensive Metabolic Panel Evaluates electrolytes (sodium, potassium, calcium, phosphorus), blood sugar, and liver function.
Albumin Low blood albumin levels suggest protein loss through damaged kidneys.
Immunoglobulin Levels IgA, IgG, and IgM levels help diagnose certain kidney diseases. Elevated IgA may suggest IgA nephropathy.
Monitoring Frequency
Testing frequency depends on disease severity and stability:
- Active disease: Weekly to monthly tests
- Stable disease: Every 3-6 months
- Remission: Every 6-12 months
Regular monitoring helps catch disease flares early, allowing prompt treatment adjustments before significant damage occurs.
Frequently Asked Questions
What autoimmune disease affects the kidneys?
Multiple autoimmune diseases can damage the kidneys. Lupus nephritis, occurring in people with systemic lupus erythematosus, is among the most common. IgA nephropathy, where IgA antibodies accumulate in kidney tissue, affects many people worldwide. Goodpasture syndrome causes antibodies to attack both kidneys and lungs.
Other conditions include membranous nephropathy, anti-GBM disease, and vasculitis affecting kidney blood vessels. Additionally, systemic conditions like scleroderma, Sjögren’s syndrome, and rheumatoid arthritis can involve kidney damage as part of their disease process.
What are the top 5 worst autoimmune diseases?
Severity varies by individual, but some autoimmune diseases pose particularly serious health threats. Systemic lupus erythematosus can attack multiple organs including kidneys, heart, brain, and lungs. Vasculitis, especially when affecting vital organs, can be life-threatening. Goodpasture syndrome rapidly damages kidneys and lungs without treatment.
Type 1 diabetes requires lifelong insulin and carries risks of severe complications. Dermatomyositis and polymyositis can affect breathing muscles and swallowing. However, “worst” is subjective—any autoimmune disease can severely impact quality of life, and modern treatments have improved outcomes for most conditions significantly.
How to live with IgA nephropathy?
Living well with IgA nephropathy involves several key strategies. Work closely with a nephrologist to monitor kidney function through regular blood and urine tests. Take prescribed medications consistently, which may include ACE inhibitors or ARBs to protect kidneys and control blood pressure. Follow dietary recommendations, which typically involve limiting sodium and potentially moderating protein intake.
Maintain a healthy weight through balanced nutrition and regular exercise. Avoid NSAIDs and other medications that stress kidneys. Monitor for signs of infection and seek prompt treatment. Some patients benefit from fish oil supplements, though you should discuss this with your doctor. Stay hydrated and avoid dehydration. Most importantly, attend all scheduled appointments and report new symptoms promptly.
How do you diagnose lupus nephritis?
Diagnosing lupus nephritis begins with recognizing kidney involvement in someone with systemic lupus erythematosus. Routine urine tests may show protein or blood, prompting further evaluation. Blood tests reveal rising creatinine, falling complement levels (C3, C4), and elevated anti-dsDNA antibodies.
However, kidney biopsy provides the definitive diagnosis and classifies lupus nephritis into one of six classes based on the pattern and severity of damage. This classification guides treatment intensity. Some patients develop nephritis early in their lupus course, while others experience kidney involvement years after their initial diagnosis. Regular screening helps catch nephritis early when treatment is most effective.
How is autoimmune kidney disease diagnosed?
Diagnosis combines clinical evaluation, laboratory testing, and often kidney biopsy. Doctors start with a thorough history and physical examination, looking for symptoms like swelling, high blood pressure, or signs of systemic autoimmune disease. Urine tests detect protein, blood, or abnormal cells.
Blood tests assess kidney function through creatinine and eGFR while checking for autoimmune markers like ANA, ANCA, anti-GBM, and complement levels. Imaging studies examine kidney structure. When these tests suggest autoimmune kidney disease but don’t provide a definitive diagnosis, kidney biopsy becomes necessary. This procedure removes a small tissue sample for microscopic examination, revealing the specific type of kidney damage and optimal treatment approach.
What are the first signs of kidney disease?
Early kidney disease often produces no symptoms, making it truly silent. When signs do appear, they may include changes in urination—foamy or bubbly urine suggesting protein loss, pink or cola-colored urine indicating blood, increased nighttime urination, or decreased output. Swelling in legs, ankles, feet, or face occurs as kidneys lose their ability to remove excess fluid. Persistent fatigue not relieved by rest is common.
Some people notice decreased appetite, nausea, or a metallic taste. However, these symptoms typically appear only after significant damage has occurred. This is why screening tests—simple urine and blood tests—are so important for people with diabetes, high blood pressure, or family history of kidney disease.
What are early warning signs of autoimmune disease?
Autoimmune diseases share certain common features, though symptoms vary by condition. Persistent fatigue that doesn’t improve with rest often appears early. Low-grade fever without clear infection suggests immune system activity. Joint pain and swelling affect many autoimmune conditions. Skin changes include rashes, particularly the butterfly-shaped rash across the cheeks in lupus.
Unexplained weight changes, either gain or loss, may occur. Digestive issues, including abdominal pain or changes in bowel habits, appear in some autoimmune diseases. Many people experience brain fog, difficulty concentrating, or memory problems. Muscle weakness or pain can develop. Since these symptoms are nonspecific and often subtle, diagnosis requires careful evaluation by healthcare providers familiar with autoimmune conditions.
What is the hardest autoimmune disease to diagnose?
Several autoimmune conditions challenge even experienced physicians. Lupus earned the nickname “the great imitator” because it mimics many other diseases and presents differently in each patient. Sjögren’s syndrome often goes undiagnosed for years since dry eyes and mouth seem like minor complaints. Early stages of vasculitis may produce vague symptoms that don’t clearly point to the diagnosis.
Some forms of autoimmune encephalitis present with psychiatric symptoms initially, leading to misdiagnosis. Addison’s disease, where the immune system attacks adrenal glands, can cause subtle symptoms for months before diagnosis. The key to diagnosing difficult autoimmune diseases lies in recognizing patterns, performing appropriate testing, and sometimes consulting specialists. Patients who persist in seeking answers despite initially negative tests often eventually receive accurate diagnoses.
What blood tests detect autoimmune diseases?
Several blood tests help identify autoimmune conditions. Antinuclear antibodies (ANA) serve as a general screening test for multiple autoimmune diseases. More specific tests include anti-dsDNA for lupus, ANCA for vasculitis, anti-GBM for Goodpasture syndrome, and rheumatoid factor for rheumatoid arthritis. Complement levels (C3, C4) help assess lupus activity. Complete blood count may show anemia or other abnormalities.
Inflammatory markers like C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) indicate active inflammation. Specific antibodies help diagnose particular conditions—anti-thyroid antibodies for Hashimoto’s thyroiditis, anti-tissue transglutaminase for celiac disease. However, no single test definitively diagnoses all autoimmune diseases. Diagnosis often requires combining test results with symptoms and clinical findings.
What are the autoimmune markers for kidney disease?
Specific autoimmune markers help identify kidney-damaging conditions. Anti-dsDNA and low complement levels (C3, C4) indicate lupus nephritis, especially when found together. ANCA antibodies suggest vasculitis affecting the kidneys—c-ANCA typically indicates granulomatosis with polyangiitis while p-ANCA suggests microscopic polyangiitis. Anti-GBM antibodies definitively diagnose anti-GBM disease and Goodpasture syndrome.
Elevated IgA levels may support IgA nephropathy diagnosis, though kidney biopsy remains necessary for confirmation. Anti-phospholipase A2 receptor antibodies appear in primary membranous nephropathy. Cryoglobulins indicate cryoglobulinemic vasculitis. Testing for these markers helps narrow the differential diagnosis, but kidney biopsy often provides the final answer regarding which specific autoimmune process is damaging the kidneys.
What are the three most common kidney diseases?
The three most prevalent kidney diseases vary by how you define “common.” Looking at chronic kidney disease causes, diabetic nephropathy (kidney damage from diabetes) ranks first, affecting millions worldwide as diabetes rates climb. High blood pressure causes the second most common kidney disease, damaging kidney blood vessels over years.
Chronic glomerulonephritis, including autoimmune forms like IgA nephropathy, represents the third major category. However, if considering acute kidney problems, acute kidney injury from medications, infections, or dehydration affects many people temporarily.
Kidney stones are extremely common, though they don’t typically cause chronic disease unless complications develop. Polycystic kidney disease, an inherited condition, affects about 1 in 500 people. Understanding these patterns helps healthcare providers screen appropriately and individuals understand their risk factors.
Conclusion
Autoimmune kidney disease represents a complex challenge, but one that modern medicine increasingly manages effectively. From lupus nephritis to IgA nephropathy, these conditions share a common thread—the immune system mistakenly attacking kidney tissue. Yet each requires individualized diagnosis and treatment approaches.
The journey with autoimmune kidney disease often begins with subtle warning signs: foamy urine, unexplained swelling, or persistent fatigue. Early detection through routine screening makes an enormous difference. Simple blood and urine tests can catch problems before irreversible damage occurs, giving treatment the best chance of preserving kidney function.
Treatment has evolved dramatically over recent decades. Powerful immunosuppressive medications now control inflammation that once inevitably progressed to kidney failure. Biologic therapies target specific immune pathways with fewer side effects than older drugs. Supportive treatments protect remaining kidney function, managing blood pressure, reducing protein loss, and addressing complications.
Living with autoimmune kidney disease requires partnership between patients and healthcare teams. Regular monitoring catches disease flares early. Medication compliance prevents progression. Lifestyle modifications—dietary changes, exercise, avoiding kidney stressors—complement medical treatment. Mental health support helps manage the emotional burden of chronic illness.
For those facing advanced disease, dialysis and transplantation offer life-sustaining options. Many transplant recipients enjoy excellent quality of life, though continued vigilance for disease recurrence remains necessary.
Prof. Aimun Ahmed and the team at Lancashire Teaching Hospitals provide comprehensive, evidence-based care for patients with autoimmune kidney disease. With over 30 years of experience and more than 5,000 patients managed, their approach combines cutting-edge medical treatment with compassionate support. Whether you’re newly diagnosed or managing long-standing disease, specialist care tailored to your individual needs provides the foundation for the best possible outcomes.
If you’re experiencing symptoms suggesting kidney problems, don’t delay seeking evaluation. If you’re living with autoimmune kidney disease, stay engaged with your care team, attend appointments, take medications as prescribed, and make lifestyle choices that protect your kidneys. Your active participation in managing your health makes a real difference in outcomes.

